
Pressure ulcers

Last Updated December 20th, 2021
Overview of pressure ulcers
Ulcers and sores are very common and may result from a wide range of environmental and clinical factors. According to recent epidemiological findings by Center for Disease Control and Prevention, about 5-10% of the global population suffer from ulcers at some point in time. A very serious form of ulcer is pressure ulcer, which is more common in bed-ridden patients. It is therefore called bed sores in many cases. The recent statistics of NCBI show that there are more than 7.4 million cases of pressure ulcers in the whole world. The elderly patients form a large section of the affected population. 28% of these patients suffer from the initial or the advanced stages of pressure ulcers. Currently it has become a major cause of permanent disability and is even reducing life expectancy in some cases.
What are pressure ulcers?
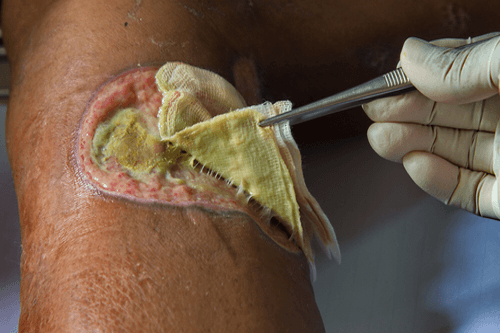
 Pressure ulcers are the localized damages of the skin and the underlying tissues that are caused by pressure and friction with a surface. These are also called pressure sores or bed sores or decubitus ulcers. Pressure ulcers result from the pressure applied to the soft tissues that obstruct blood flow to those tissues. Pressure ulcers are more common in people, particularly the aged people who lead a sedentary lifestyle. Patients confined to the bed or wheelchair due to some serious diseases have the likelihood of developing pressure ulcers. A number of other dietary, environmental and clinical factors may also contribute to these types of ulcers. The areas that are commonly affected in such conditions are- the back of shoulders, back of the cranium, pelvic region, elbows, knees and ankles. Most affected are the overlying skin of sacrum, coccyx, heels and the hips.
Pressure ulcers are the localized damages of the skin and the underlying tissues that are caused by pressure and friction with a surface. These are also called pressure sores or bed sores or decubitus ulcers. Pressure ulcers result from the pressure applied to the soft tissues that obstruct blood flow to those tissues. Pressure ulcers are more common in people, particularly the aged people who lead a sedentary lifestyle. Patients confined to the bed or wheelchair due to some serious diseases have the likelihood of developing pressure ulcers. A number of other dietary, environmental and clinical factors may also contribute to these types of ulcers. The areas that are commonly affected in such conditions are- the back of shoulders, back of the cranium, pelvic region, elbows, knees and ankles. Most affected are the overlying skin of sacrum, coccyx, heels and the hips.
What causes pressure ulcers?
There are three underlying mechanisms that induce the formation of pressure ulcers. These are-
- External pressure: External pressure exerted on the bony outgrowths causes compression of the blood vessels in that area. This results in obstructed circulation through the capillaries, which in turn results in deficient oxygen supply to the adjoining tissues. The following conditions arise in such cases-
- Ischemia: Dearth of blood
- Hypoxia: Low oxygen level
- Oedema: Swelling of tissues
- Inflammation
- Necrosis
- Ulcer formation
- Friction: Continuous friction with a surface affects the blood vessels present directly below the skin. This leads to ulcer formation on the elbows and the back.
- Shear: In this condition, a visible separation of the skin from the underlying tissues occur, wherein the underlying tissues tend to move downward whenever a person tries to get up from the bed and carry out any sort of movement.
There are a few other factors that precipitate the formation of pressure ulcers. These are listed below-
- Malnutrition (protein and calorie deficiency)
- Wetness of the skin due to perspiration or incontinence (microclimate)
- Arteriosclerosis (reduced blood flow to the skin)
- Neuropathy or paralysis (reduces sensation in the skin)
- Peripheral Vascular Disease
- Hypotension
- Cerebral Vascular
- Diabetes Mellitus
- Tobacco smoking
- Overuse of anti-inflammatory drugs
- Prolonged stay in humid and sultry environments
- Low BMI (Body Mass Index)
- Dry skin
- Immobility (temporary or permanent)
- Altered mental condition
- Bowel or urinary incontinence
- History of ulcers and sores
How do you classify pressure ulcers?
The classification of pressure ulcers is done mainly based on the stage of the disease. These are elucidated below-
- Stage I: In this type, only the epidermis is affected. A localized reddish patch appears over any bony prominence. Pigmentation appears in the later stages along with a palpable change in the temperature, thickness and texture of the affected skin. In people with a dark complexion, these changes are not so visible.
- Stage II: The dermis is affected in this case. It is characterized by a loss of thickness of the dermis and the emergence of a shallow open ulcer with a reddish or pinkish wound bed (devoid of the slough). Fluid-filled blisters may gradually appear, which rupture in the later stages, releasing the content.
- Stage III: Major tissue loss (full-thickness loss) occurs in this case. The subcutaneous fat is exposed and tunnelling may be observed. This stage is more prominent in areas of high adiposity.
- Stage IV: The bones, tendons and the muscles are exposed in this case. A thickened slough may appear on some parts of the wound. The characteristic features of this stage are the tunnelling and the undermining of the subcutaneous tissues. The ulcers can even penetrate into the muscles, tendons, joint capsules or fascia. This increases the risks of osteomyelitis.
- Unstageable: Here, the stage cannot be determined easily since a major depth of the wound is covered by slough. The depth and stage of the wound (ulcer) can be determined only after removing the slough completely.
- Suspected deep tissue injury: This is characterised by a purplish area of discoloured skin (with no breaks) and blood-filled blisters, both arising from pressure and shear stress. The affected tissues are tender, warm and painful compared to the adjoining tissues. This type of deep tissue injury is difficult to detect in individuals with dark complexion. In the advanced stages, slough may form on the wound bed or more layers of underlying tissues may be exposed.
Another classification of ulcers done based on the areas affected is given below-
- Epidermal
- Dermal
- Sub-cutaneous tissue
- Muscle
- Bone
Treatment & prevention
 Repositioning the patient is the first course of action in case the bed-ridden patient has developed pressure ulcers. Special mattresses, pillows, and cushions can be used that enables one to sit and rest without making the body susceptible to bedsores. The dressing should be regularly changed so that it doesn’t get infected. In case of spinal cord injury patients who are bed rest, electric stimulation can be used to treat the ulcers. Vacuum- associated suction can also be used to clean the ulcers.
Repositioning the patient is the first course of action in case the bed-ridden patient has developed pressure ulcers. Special mattresses, pillows, and cushions can be used that enables one to sit and rest without making the body susceptible to bedsores. The dressing should be regularly changed so that it doesn’t get infected. In case of spinal cord injury patients who are bed rest, electric stimulation can be used to treat the ulcers. Vacuum- associated suction can also be used to clean the ulcers.
In order to prevent the formation of pressure ulcers, the temperature and moisture levels of the patient’s room can be maintained at an optimal level that prevents drying of skin. One should not apply heating pads on areas where pressure ulcers can develop. It is better to wear silk or similar to silk fabrics instead of cotton or cotton blends in order to prevent friction. These can be also be prevented by using prophylactic dressing on bony projections.
- https://www.ncbi.nlm.nih.gov/pubmedhealth/PMHT0025824/
- https://medlineplus.gov/pressuresores.html
- https://www.ahrq.gov/professionals/systems/hospital/pressureulcertoolkit/putool3.html
- https://www.gov.uk/government/publications/pressure-ulcers-applying-all-our-health
- https://www.mayoclinic.org/diseases-conditions/bed-sores/symptoms-causes/syc-20355893
Dos and Don'ts
Dos
- When taking care of a bed-ridden person who is likely to develop bed sores, it is important to turn the patient once every two hours.
- Regularly check for signs of ulceration on the skin for bed-ridden patients.
- Moisturize and massage dry skin regularly, especially areas which remain stationary.
Don'ts
- Keep the head of the bed of the patient at an angle greater than 30 degrees.
- Drag the patient too much while moving him/her. This creates friction and results in inflammation and ulceration of the skin.
- Use thick dressing over the ulcer wounds. Also, avoid using a lot of padding to put under the patient. Any sort of thick covering or padding will increase pressure ulcers.
Help Others Be Fit
Related Conditions




Trending Topics
































































































































About
Related Conditions
Subscribe to free FactDr newsletters.
REVAMP YOUR
LIFE
HEALTH
WELLNESS

If you're enjoying our website, we promise you'll absolutely love our new posts. Be the first one to get a copy!
Get factually correct, actionable tips delivered straight to your inbox once a week.
We hate spam too. We will never share your email address with anyone. If you change your mind later, you can unsubscribe with just one click
By clicking Subscribe, I agree to the FactDr Terms & Conditions & Privacy Policy and understand that I may opt out of FactDr subscriptions at any time.
×
How can we improve it?
×
Happy to know you loved our article!
Did it give you information that you used / can use in your life?

