
Hyperkalemia

Last Updated December 20th, 2021
Overview
The human body requires potassium in order to perform many of its vital functions. This mineral is an essential component of the sodium-potassium ion pump that helps generate electrical impulses in nerve cells and drive other critical cellular functions. However, the level of potassium must be maintained within a healthy range. It is the function of the kidneys to ensure this. An abnormal increase of potassium level in the blood is known as hyperkalemia. Mild fluctuations do not normally produce any adverse symptoms. However, an extreme imbalance can have severe consequences including paralysis, irregular heart rhythm, and even heart failure.
Definition
 ‘Hyperkalemia’ refers to elevated levels of potassium in the blood.
‘Hyperkalemia’ refers to elevated levels of potassium in the blood.
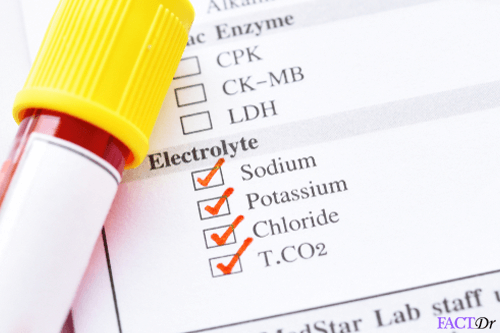
A normal blood potassium level ranges from 3.5 to 5mEq/L (milliequivalents per liter) in adults.
When the level of blood potassium lies between 5.1 to 6.0 mEq/L it is considered to indicate mild hyperkalemia. 6.1 to 7.0 mEq/L is considered moderate hyperkalemia. When the level of potassium in the blood exceeds this figure it is considered to be a case of severe hyperkalemia.
This can result either from excessive intake of potassium or from an insufficient elimination of excess electrolyte. Hyperkalemia may also occur in the event of major injuries involving significant hemolysis or breakdown of red blood cells which causes them to release potassium into the bloodstream. Since the regulation of blood electrolytes is primarily managed by the kidneys, any imbalance is normally associated with some form of disturbance in kidney function.
Causes
The amount of potassium than a normal diet offers usually exceeds the body’s requirements. As much as 90% of this excess potassium is eliminated by the kidneys through the urine. Hence, in 3 out of 4 cases, hyperkalemia is brought about by the failure of the kidneys. It is also associated with adrenal insufficiency. This is an endocrine disorder in which the adrenal glands fail to produce adequate quantities of the hormone aldosterone which is responsible for regulating the elimination of potassium through the urine. Hyperkalemia can also be brought on by any condition that causes extensive lysis or breakdown of red blood cells. A fuller list of possible causes is provided below.
- Renal disorders such as chronic kidney disease or kidney failure. Those who have received kidney transplants are also at an increased risk of developing hyperkalemia.
- Adrenal gland disorders such as Addison’s disease.
- Taking certain medications.
- Dehydration.
- Excess intake of potassium supplements.
- HIV infection.
- Large burns or significant injuries causing the breakdown of red blood cells which then release the potassium contained in them.
- Severe trauma leading to significant muscle damage.
- Blood transfusion.
- Diabetic ketoacidosis.
- Medical conditions such as Gordon’s syndrome.
Symptoms
Patients with mildly elevated potassium levels in the blood may be entirely asymptomatic or the symptoms may be subtle and nonspecific.
This makes it difficult to diagnose the condition accurately. Symptoms may be slow to appear if the potassium content in the blood rises gradually rather than suddenly.
Potassium is mainly involved in generating nerve impulses and regulating muscular activity, most notably with regard to the heart and digestive system.
Hence it is these functions that are directly affected when blood potassium levels exceed the normal limits to a significant degree.
- Weakness and fatigue.
- Heart palpitations.
- Paralysis.
- Difficulty in breathing.
- Nausea or vomiting.
- Chest pain.
- Tingling or pricking sensation.
Clinical Complications
Potassium directly influences the electrical impulses that control heart contractions. Hence, severe hyperkalemia is typically associated with significant cardiac consequences. Rapid bursts of heart activity (fibrillation) can lead to cardiac arrest. The disturbance in normal electrical activity associated with cardiac muscles may also cause the heart to slow down or totally flatline.
Diagnosis
Diagnosing hyperkalemia can be challenging. Blood tests showing elevated levels of potassium in the blood may not be conclusive and may have to be repeated. This is because the process of collecting the blood sample can itself sometimes lead to rupture of red blood cells causing a false elevation of potassium content in the readings. This is known as pseudohyperkalemia. However, if the symptoms displayed by the patient are consistent with those of abnormally elevated levels of potassium in the blood, the blood test may be repeated, accompanied by urine tests to confirm the results.
The physician may be alerted to the possibility of hyperkalemia by examining the patient’s medical history to check for any medications that may have disturbed kidney function, other medical conditions that could trigger abnormal levels of potassium in the blood or for significant injuries that might also be responsible for hyperkalemia. Since the primary complication associated with hyperkalemia is abnormal heart rhythm and weak pulse, an electrocardiogram is usually necessary to assess heart function. However, it is widely acknowledged in clinical practice that this is not necessarily conclusive. Severe cases of hyperkalemia have been known to present without any suspicious heart activity.
Treatment and prevention
 Treatment – Treatment for hyperkalemia must be individualized based upon the underlying cause of hyperkalemia, the severity of the symptoms, or appearance in the ECG change, and the overall health status of the patient. Treatment may include any one of the following or a combination of methods
Treatment – Treatment for hyperkalemia must be individualized based upon the underlying cause of hyperkalemia, the severity of the symptoms, or appearance in the ECG change, and the overall health status of the patient. Treatment may include any one of the following or a combination of methods
- Low potassium diet for the patient (in minor cases)
- Discontinue medications that can increase the blood potassium level.
- Sodium bicarbonate administration to counteract acidosis and to promote movement of potassium from the extracellular space back into the cells.
- Medications known as cation-exchange resins, which bind potassium and lead it to excretion through the gastrointestinal tract.
- Intravenous calcium to protect the heart and the muscles from the effects of hyperkalemia.
- Intravenous administration of glucose and insulin, which promotes the movement of potassium from the extracellular space between the cells.
- Dialysis, particularly if other measures have failed in case of renal failure.
Prevention
- Follow a low potassium diet if needed – Make sure to ask your healthcare specialist or dietitian about the quantity of potassium that is right for you. Eating too much can be harmful and having a little can cause problems.
- Try avoiding certain salt substances – Certain salt substances are high in potassium levels. Those with a kidney disease should avoid them.
- Avoid herbal remedies and supplements – Make sure to consult your healthcare specialist to know if the herbal remedy that you wish to take does not increase potassium levels.
- Take water pills or potassium binders – Some people may need to remove the extra potassium that is present in their body and make sure that it does not come back.
- https://www.ncbi.nlm.nih.gov/books/NBK470284/
- https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-14/fourteen-thirteen
- http://cjasn.asnjournals.org/content/early/2012/05/16/CJN.01150112.full
- https://www.kidney.org/atoz/content/hyperkalemia/facts
- https://www.aafp.org/afp/2006/0115/p283.html
Dos and Don'ts
Dos
- Make sure to have your medications exactly as prescribed.
- Have low potassium foods.
- Discontinue any oral supplements of potassium.
Don'ts
- Indulge in any strenuous activities.
- Use a salt substitute without consulting your doctor.
- Consume yam, sweet potatoes, kidney beans, avocado, bananas, fig, kiwis etc. as they are high in potassium.
Help Others Be Fit
Related Conditions

Trending Topics































































































































About
Related Conditions


Subscribe to free FactDr newsletters.
REVAMP YOUR
LIFE
HEALTH
WELLNESS

If you're enjoying our website, we promise you'll absolutely love our new posts. Be the first one to get a copy!
Get factually correct, actionable tips delivered straight to your inbox once a week.
We hate spam too. We will never share your email address with anyone. If you change your mind later, you can unsubscribe with just one click
By clicking Subscribe, I agree to the FactDr Terms & Conditions & Privacy Policy and understand that I may opt out of FactDr subscriptions at any time.
Test Your Knowledge
×
How can we improve it?
×
Happy to know you loved our article!
Did it give you information that you used / can use in your life?

